Most Tubular Reabsorption Occurs In The
Juapaving
Mar 19, 2025 · 5 min read
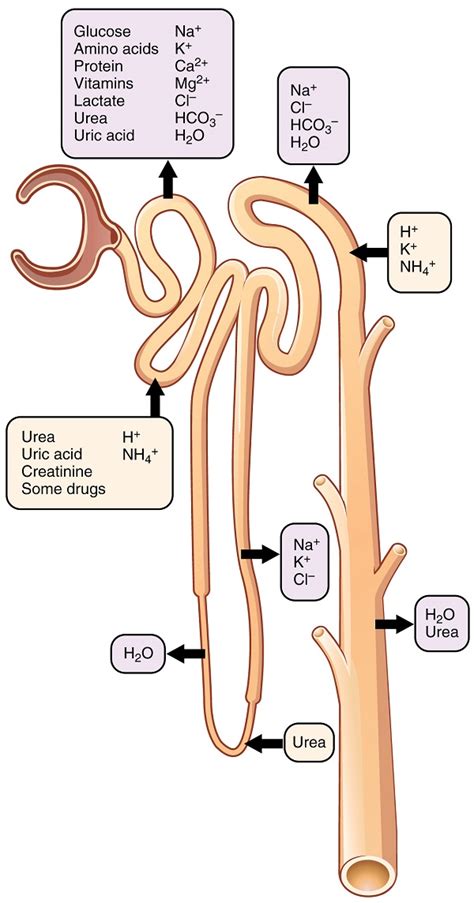
Table of Contents
Most Tubular Reabsorption Occurs in the Proximal Convoluted Tubule: A Deep Dive into Renal Physiology
The kidneys are remarkable organs responsible for maintaining homeostasis by filtering blood, removing waste products, and regulating fluid balance. This intricate process involves several key steps, including glomerular filtration, tubular reabsorption, and tubular secretion. While all three are crucial, the majority of reabsorption—the process of reclaiming essential substances from the filtrate—occurs in a specific segment of the nephron: the proximal convoluted tubule (PCT). This article will delve into the detailed mechanisms and significance of this vital process.
The Nephron: The Functional Unit of the Kidney
Before exploring the PCT's role, it's essential to understand the nephron's structure. The nephron, the functional unit of the kidney, is a complex structure composed of several key components:
-
Renal Corpuscle: This structure comprises the glomerulus (a network of capillaries) and Bowman's capsule (a cup-like structure surrounding the glomerulus). Glomerular filtration occurs here.
-
Proximal Convoluted Tubule (PCT): This is the longest segment of the nephron and is where the majority of reabsorption takes place.
-
Loop of Henle: This loop dips into the renal medulla and plays a crucial role in concentrating urine.
-
Distal Convoluted Tubule (DCT): This segment is involved in fine-tuning electrolyte balance and responding to hormonal regulation.
-
Collecting Duct: Several nephrons drain into a single collecting duct, which further modifies the filtrate before it becomes urine.
The Proximal Convoluted Tubule: The Reabsorption Powerhouse
The PCT's unique structure and cellular mechanisms are perfectly adapted for mass reabsorption. Its epithelial cells possess several features crucial for this process:
-
Extensive Brush Border: The apical surface (facing the lumen) of PCT cells is covered with numerous microvilli, forming a brush border. This dramatically increases the surface area available for reabsorption.
-
Abundant Mitochondria: The high metabolic activity required for active transport is supported by a dense population of mitochondria within PCT cells. Reabsorption is an energy-intensive process.
-
Tight Junctions: These junctions between adjacent cells create a selective barrier, regulating the passage of substances between cells.
Mechanisms of Reabsorption in the PCT
Reabsorption in the PCT involves several distinct mechanisms, both active and passive:
1. Sodium Reabsorption: The Driving Force
Sodium (Na+) reabsorption is the primary driving force for many other reabsorption processes. Na+ is actively transported across the basolateral membrane (facing the interstitial fluid) via the Na+/K+ ATPase pump. This creates a low intracellular Na+ concentration, establishing a concentration gradient that drives Na+ entry from the lumen across the apical membrane.
Different transport mechanisms are involved in apical Na+ entry:
-
Secondary Active Transport: Na+ co-transport with glucose, amino acids, and phosphate occurs via specific transporters. The energy stored in the Na+ gradient powers the uptake of these vital nutrients.
-
Na+/H+ Exchange: Na+ enters the cell while H+ is extruded into the lumen. This is important for acid-base balance.
2. Water Reabsorption: Following Sodium
Water reabsorption is predominantly passive and follows the osmotic gradient established by Na+ reabsorption. As Na+ is reabsorbed, the osmolarity of the interstitial fluid increases, drawing water across the PCT epithelium via aquaporin channels (water channels) in the apical and basolateral membranes.
3. Glucose and Amino Acid Reabsorption: Complete Reabsorption
Glucose and amino acids are completely reabsorbed in the PCT under normal physiological conditions. This is achieved via secondary active transport coupled with Na+ reabsorption. The transporters have a limited capacity, and if the filtered load exceeds this capacity (e.g., in diabetes mellitus), glucose and amino acids will appear in the urine (glycosuria and aminoaciduria).
4. Phosphate Reabsorption: Regulated Process
Phosphate reabsorption is also coupled to Na+ transport but is subject to hormonal regulation. Parathyroid hormone (PTH) inhibits phosphate reabsorption.
5. Bicarbonate Reabsorption: Acid-Base Balance
Bicarbonate (HCO3-) reabsorption is essential for maintaining acid-base balance. It's indirectly reabsorbed through a complex process involving carbonic anhydrase, an enzyme that catalyzes the conversion of CO2 and H2O to H+ and HCO3-.
6. Potassium Reabsorption and Secretion: Fine-tuning
Potassium (K+) reabsorption and secretion occur in the PCT, but the net effect is generally reabsorption. The precise balance depends on several factors, including dietary K+ intake and hormonal influences.
7. Urea Reabsorption: Passive Process
Urea, a waste product of protein metabolism, is passively reabsorbed in the PCT. The extent of reabsorption is influenced by the concentration gradient and permeability of the PCT epithelium.
8. Chloride Reabsorption: Passive and Active
Chloride (Cl-) reabsorption occurs both passively, following the electrical gradient created by Na+ reabsorption, and actively through specific transporters.
Quantitative Aspects of PCT Reabsorption
The PCT's role in reabsorption is truly remarkable. Approximately 60-70% of the glomerular filtrate's volume is reabsorbed in the PCT. This includes almost all of the filtered glucose, amino acids, and bicarbonate, as well as a substantial portion of sodium, water, potassium, chloride, and other solutes. This efficient reabsorption is vital for conserving essential nutrients and maintaining fluid balance.
Clinical Significance of PCT Dysfunction
Impaired PCT function can have significant clinical consequences. Conditions affecting the PCT can lead to:
-
Fanconi Syndrome: A group of disorders characterized by generalized proximal tubule dysfunction, resulting in the urinary excretion of glucose, amino acids, phosphate, and bicarbonate.
-
Metabolic Acidosis: Impaired bicarbonate reabsorption can cause metabolic acidosis, a condition characterized by a low blood pH.
-
Electrolyte Imbalances: Disrupted reabsorption of electrolytes can lead to various electrolyte imbalances, potentially causing serious complications.
Conclusion
The proximal convoluted tubule is the undisputed champion of tubular reabsorption. Its unique structural features and sophisticated transport mechanisms allow for the efficient reabsorption of a vast array of substances, playing a crucial role in maintaining homeostasis. Understanding the physiology of the PCT is vital for comprehending renal function and appreciating the complexities of fluid and electrolyte balance. Further research continues to unravel the intricacies of this fascinating segment of the nephron, furthering our understanding of kidney function and disease. The remarkable efficiency of the PCT highlights the body's intricate design and the importance of maintaining its health. Disruptions to this vital process have far-reaching consequences, emphasizing the critical role the PCT plays in overall health.
Latest Posts
Latest Posts
-
What Planet Is Called The Red Planet
Mar 19, 2025
-
What Is Xlvi In Roman Numerals
Mar 19, 2025
-
How Many Inches Are 20 Cm
Mar 19, 2025
-
Least Common Multiple Of 12 And 20
Mar 19, 2025
-
How Many Yards Is 300 Ft
Mar 19, 2025
Related Post
Thank you for visiting our website which covers about Most Tubular Reabsorption Occurs In The . We hope the information provided has been useful to you. Feel free to contact us if you have any questions or need further assistance. See you next time and don't miss to bookmark.
